
The Revenue Cycle Breakdown Nobody Owns—Until Cash Stops Moving
In every practice, there are "No Man's Lands"—gray areas between the front desk, clinical team, and billing office. These are the cracks where authorizations vanish, coding queries die, and revenue disappears. Discover the four most common accountability gaps and how to assign ownership before your cash flow stalls.
January 15, 2026
Revenue Cycle Management (RCM) is not a solo sport; it is a relay race.
In a relay race, the most dangerous moment isn't when the athlete is sprinting at full speed; it is the split second when they pass the baton to the next runner. If the handoff is fumbled, it doesn't matter how fast the runners are—the race is lost.
In your medical practice, your "baton" is the patient's claim.
- The Front Desk starts the race (Registration).
- The Clinical Team runs the middle leg (Documentation).
- The Billing Team sprints to the finish line (Submission & Collection).
When these departments operate in silos, they often perform their individual sprints perfectly but drop the baton during the handoff. The front desk smiles at the patient. The doctor documents the care perfectly. The biller submits the claim on time.
Yet, the claim is denied. Or worse, it vanishes.
Why? Because the error didn't happen in a department; it happened between them. These are the "No Man's Lands"—the gray areas of accountability where tasks slip through the cracks because "everybody thought somebody else was doing it."
Below, we identify the four most common accountability gaps in a medical practice and how to assign ownership before your cash flow stalls.
Gap #1: The Authorization Abyss (Front Desk vs. Clinical)
This is the single most expensive gap in any specialty practice. An authorization denial is almost always a "hard denial"—meaning it cannot be appealed. If you perform a $20,000 surgery without a prior auth number, that $20,000 is gone forever.
The Scenario
A patient comes in for a consultation. The doctor decides they need a specific procedure (e.g., an MRI or a joint injection) and schedules it for next week.
The Breakdown
- The Front Desk thinks: "I checked the patient's insurance eligibility, so we are good. The clinical team knows what procedure is being done, so they will handle the specific authorization."
- The Clinical Team thinks: "I'm just the nurse/MA. I don't handle insurance. The front desk took the card, so they must have cleared it."
Because both sides assume the other owns it, nobody logs into the portal to request the auth. The patient shows up, the procedure is performed, and 30 days later, the denial arrives.
The Fix: The "Gatekeeper" Rule
You cannot rely on assumptions for authorizations. You need a hard stop.
- Assign Ownership: Designate one person (e.g., the Surgical Coordinator or Referral Coordinator) whose sole job is to secure auths.
- The Process Check: Implement a policy where the procedure cannot be scheduled in the calendar until the Auth Number is entered into a mandatory field. If the field is blank, the appointment doesn't exist.
Gap #2: The "Pending" Purgatory (The Silent Killer)
Most billing teams are trained to be "firefighters." They wake up every morning and look at the Denial Report. They see what was rejected and they fight to fix it.
But what about the claims that aren't rejected? What about the claims that are just... silent?
The Scenario
A biller submits a batch of 50 claims. 45 are paid. 3 are denied. The biller works the 3 denials.But what happened to the other 2?
Maybe the clearinghouse dropped them. Maybe the payer "lost" them. Maybe they are stuck in a "pending adjudication" status for 120 days.
The Breakdown
This is a classic ownership gap because these claims don't appear on standard "To-Do" lists.
- The Biller is looking at the "Denied" bucket.
- The Payment Poster is looking at the "Paid" bucket.
- Nobody owns the "No Response" bucket.
These claims sit in purgatory. They age silently from 30 days to 60, to 90, to 180. By the time someone notices them, the Timely Filing limit has passed, and the revenue is lost.
The Fix: The "No Response" Protocol
You need to treat "No Response" as an active denial.
- Assign Ownership: Create a recurring task for a specific biller: "Every Tuesday, run a report of all claims >45 days with $0 payment and no denial code."
- The Action: The biller must call the payer or check the portal status for these specific claims. Usually, simply re-submitting them solves the problem, but someone has to notice they are missing first.
Gap #3: The Provider Query Standoff (Billing vs. Providers)
This gap is arguably the most politically sensitive one in the practice. It occurs when a claim cannot be billed because the documentation is incomplete, ambiguous, or unspecific.
The Scenario
A provider dictates a note for a "Laceration Repair." The biller reviews it and realizes the provider didn't specify the length of the laceration (e.g., 2.5cm vs 7.0cm). Without that length, the biller cannot choose the correct CPT code.
The Breakdown
The claim enters the "Coding Query" bucket. This is where revenue goes to hibernate.
- The Biller sends a message to the provider. They don't want to "nag" the doctor, so they send one email and wait.
- The Provider is seeing 30 patients a day. They view billing queries as "admin fluff" that can wait until the weekend.
Weeks pass. The biller doesn't want to overstep their authority by pestering the boss, so the claim sits on "Hold." Eventually, to clear the queue, someone might arbitrarily pick a lower-level code (downcoding) just to get it out the door, costing the practice revenue. Or worse, it hits the timely filing limit and is written off entirely.
The Fix: The "72-Hour Rule"
You need a formalized escalation process that removes emotion from the equation.
- The Agreement: Establish a policy that all coding queries must be answered within 72 hours.
- The Escalation: If a query is pending for >5 days, it automatically triggers a report to the Medical Director or Practice Administrator. This isn't about "tattling"; it's about protecting the practice's income. The biller isn't nagging; the protocol is nagging.
Gap #4: The Patient Balance Void (Front Desk vs. Billing)
Who is responsible for collecting the $75.00 outstanding balance from the patient's previous visit?
The Scenario
Mrs. Smith arrives for her appointment. She has a balance of $150 from her last visit (her deductible). She checks in at the front desk.
The Breakdown
- The Front Desk sees their role as "Customer Service." They want the patient to be happy. Asking for $150 feels confrontational and awkward. They think, "The billing department sends statements; let them handle it."
- The Billing Team is sitting in a back office (or another state). They have no leverage. They can send paper statements, but paper statements have a 20% success rate. The only time you have leverage is when the patient is standing in front of you.
Because the front desk avoids the "money talk" and the billing team lacks physical access, the balance grows.
The Fix: The "Check-In" Audit
You must empower (and mandate) the front desk to collect previous balances.
- The Tool: Give the front desk a script. "Mrs. Smith, I see a balance of $150. How would you like to take care of that today? The card on file?"
- The Metric: Measure "Point-of-Service (POS) Collections" as a KPI for the front desk staff, not the billing staff. If the patient walks past the front desk without paying a known balance, that is a front-desk failure, not a billing failure.
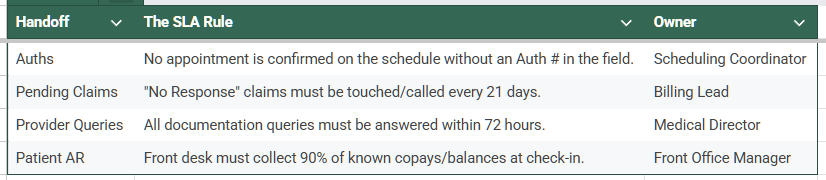
The Solution: Internal Service Level Agreements (SLAs)
How do you close these gaps? You stop treating your practice as a "family" and start treating it as a business with internal contracts.
In the corporate world, these are called Service Level Agreements (SLAs). An SLA defines exactly what needs to be done, who does it, and when it must be finished.
The "Hub" Role
Finally, someone must referee these SLAs. This is typically the Practice Administrator or an external Revenue Cycle Manager. Their job is not to do the work, but to police the handoffs. They are the ones who look at the weekly report and say, "Dr. Jones, you have 15 unanswered queries," or "Front Desk, we missed 4 auths this week."
Conclusion
Revenue leakage rarely happens because of a single catastrophic error. It happens in the quiet moments—the unanswered email, the unassigned task, the assumption that "someone else" is handling it.
If your cash flow is stalling, don't just blame the billers. Look at the handoffs. Look at the gray areas between your departments.
Is your practice suffering from the "Bystander Effect"? We specialize in connecting the dots. We don't just process claims; we audit your entire workflow to identify where accountability is breaking down. Contact Us Today for a Workflow Analysis and let’s get your team running like a relay, not a scramble.
Ready to reduce Your Aging AR
Get a no-pressure AR review and see exactly where recoveries can happen fast.
We’ll show you the gaps, the opportunities, and the impact ARaura can make in your next billing cycle.